SOLICITE JÁ!
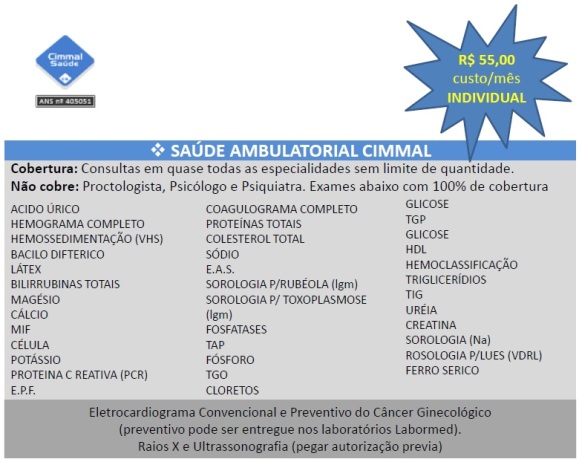
PLANO DE SAÚDE AMBULATORIAL CIMMAL
Nome
*
T
el.:
*
..
Cel.:
*
....
E-mail
*
.
INFORMAÇÕES ADICIONAIS:
*